
Most Australians experience gut symptoms at some point. When things are not going so well it is essential to check in with your general practitioner for a comprehensive evaluation. Many gastrointestinal conditions are well managed by your GP, but some symptoms may require the input of a specialist gastroenterologist.
Here’s a guide for patients in Melbourne and beyond to understanding where your symptoms sit and when a gastroenterology referral may be warranted.
What Can My GP Manage Without a Specialist Referral?
General practitioners are trained to diagnose and treat the majority of gastrointestinal conditions.
Reflux and heartburn
If you have typical reflux symptoms such as a burning sensation in the chest, regurgitation, or symptoms that worsen after meals or lying down, your GP will often recommend lifestyle changes and a trial of medication. Most people improve within six to eight weeks, but persistent symptoms may require further assessment.
Functional dyspepsia and bloating
Unexplained upper abdominal discomfort, early fullness, or persistent bloating is common. If positive for Helicobacter pylori (a stomach bacteria), a trial of first line treatment is warranted. Many people respond well at this stage.
Irritable bowel syndrome (IBS)
IBS is one of the most common gut conditions in Australia. Your GP can diagnose it using established clinical criteria, provided there are no concerning features, and guide you through dietary changes including a low FODMAP approach with a dietitian, as well as first-line treatments.
Constipation
Lifestyle factors, diet, and medications are the most common culprits, and your GP can address these effectively.
When Should You See a Gastroenterologist?
Some symptoms, patterns, or circumstances mean a gastroenterologist’s involvement is worthwhile. If you are based in Melbourne, a referral to a gastroenterology clinic at a public hospital or a private gastroenterologist from your GP is the usual starting point.
Symptoms that haven’t resolved with treatment
If reflux persists after eight weeks of adequate medication, or IBS symptoms continue to significantly affect your quality of life despite first-line management, it’s reasonable to explore what’s driving them.
You’re over 50 and experiencing new gut symptoms
Further investigation, typically an endoscopy or colonoscopy, may be recommended to rule out structural causes. Earlier investigation may be appropriate depending on your personal or family history.
Unexplained changes in bowel habit
A persistent shift in your bowel pattern, especially if associated with other symptoms, may warrant further evaluation.
Chronic diarrhoea
Diarrhoea lasting more than two weeks, or that keeps returning, is not something to normalise or wait out. There are many possible causes, from infections and food intolerances through to inflammatory bowel disease and other conditions and identifying the right one matters for treatment.
Confirmed or suspected coeliac disease
If blood tests suggest coeliac disease, a gastroscopy with biopsy is needed to confirm the diagnosis. It’s important not to start a gluten-free diet before this, as doing so can affect the accuracy of testing.
A raised faecal calprotectin
This is a stool test your GP can order that measures inflammation in the gut. An elevated result doesn’t automatically mean something serious, but it does suggest that further investigation with a gastroenterologist is the next step.
Suspected inflammatory bowel disease (IBD)
Crohn’s disease and ulcerative colitis are chronic inflammatory conditions that require specialist diagnosis and management. Symptoms that may suggest IBD include ongoing diarrhoea with or without blood or mucus, abdominal pain, unintended weight loss, and perianal symptoms. IBD can be subtle, and it’s not uncommon for there to be a delay between symptom onset and diagnosis.
Bowel cancer screening
Australia has a national bowel cancer screening program that sends home testing kits to eligible adults. A positive result requires a follow-up colonoscopy. Your GP will refer you, and a gastroenterologist will perform and interpret the procedure.
Do Gastroenterologists Treat Liver Conditions?
Gastroenterologists manage conditions affecting not just the bowel but also the liver, which is one of the body’s most metabolically active organs. Liver disease often develops silently, without obvious symptoms in the early stages, which is why abnormal blood test results or incidental imaging findings are common starting points for referral.
Abnormal liver function tests
Liver function tests (LFTs) are a routine part of blood panels and are often checked by GPs in the context of fatigue, medication reviews, or general health assessments. Persistently elevated or unexplained results warrant specialist input to identify the underlying cause, which may range from alcohol and fatty liver through to autoimmune conditions, viral hepatitis, or medication effects.
Fatty liver disease
Metabolic dysfunction-associated fatty liver disease (sometimes still called non-alcoholic fatty liver disease) is now one of the most common liver conditions in Australia, affecting up to one in three adults. It is closely linked to metabolic risk factors including obesity, type 2 diabetes, high cholesterol, and high blood pressure. In many cases it is picked up incidentally on an ultrasound or through blood tests. Most people have no symptoms. While early stages are managed with lifestyle changes, specialist input is important for assessing the degree of liver involvement and identifying those at risk of progression.
Hepatitis B and hepatitis C
Chronic hepatitis B and C are viral infections that cause ongoing liver inflammation and, over time, can lead to cirrhosis and liver cancer if unmanaged. Both conditions can be present for years without causing noticeable symptoms. Hepatitis C is now curable with a short course of oral medication. Hepatitis B requires ongoing monitoring and, in some cases, long-term antiviral treatment. If you have been diagnosed with either, or have risk factors and haven’t been tested, a gastroenterologist or hepatologist can guide appropriate assessment and management.
Jaundice
Yellowing of the skin or whites of the eyes (jaundice) occurs when bilirubin, a yellow pigment produced by the breakdown of red blood cells, builds up in the body. It can reflect problems with the liver, bile ducts, or blood cells and always requires prompt investigation to determine the cause. If your GP identifies jaundice, they will arrange urgent assessment.
Established liver disease and cirrhosis
If you have a known diagnosis of liver disease at any stage, regular specialist review is part of standard care. Monitoring aims to detect complications early and assess whether the condition is stable or progressing.
Which Symptoms Need Prompt Attention?
The following symptoms should prompt you to see your GP soon. Not because they are always serious, but because they need timely investigation to determine the cause. Unexplained iron deficiency or anaemia, blood in your stool or black and tarry stools, difficulty swallowing especially with solid food, unintentional weight loss, persistent vomiting, yellowing of the skin or eyes, and a lump or fullness in your abdomen all fall into this category.
If you notice any of these, please don’t wait. Book an appointment with your GP promptly and let them know specifically what you’ve noticed.
What Is the Difference Between a Public Hospital and a Private Gastroenterologist in Melbourne?
If your GP refers you to a private gastroenterologist rather than a public hospital, this may be deliberate. It’s worth understanding why.
Public hospital gastroenterology services triage referrals by urgency. Patients with the most pressing clinical needs are prioritised, and those with less urgent presentations can wait a considerable time.
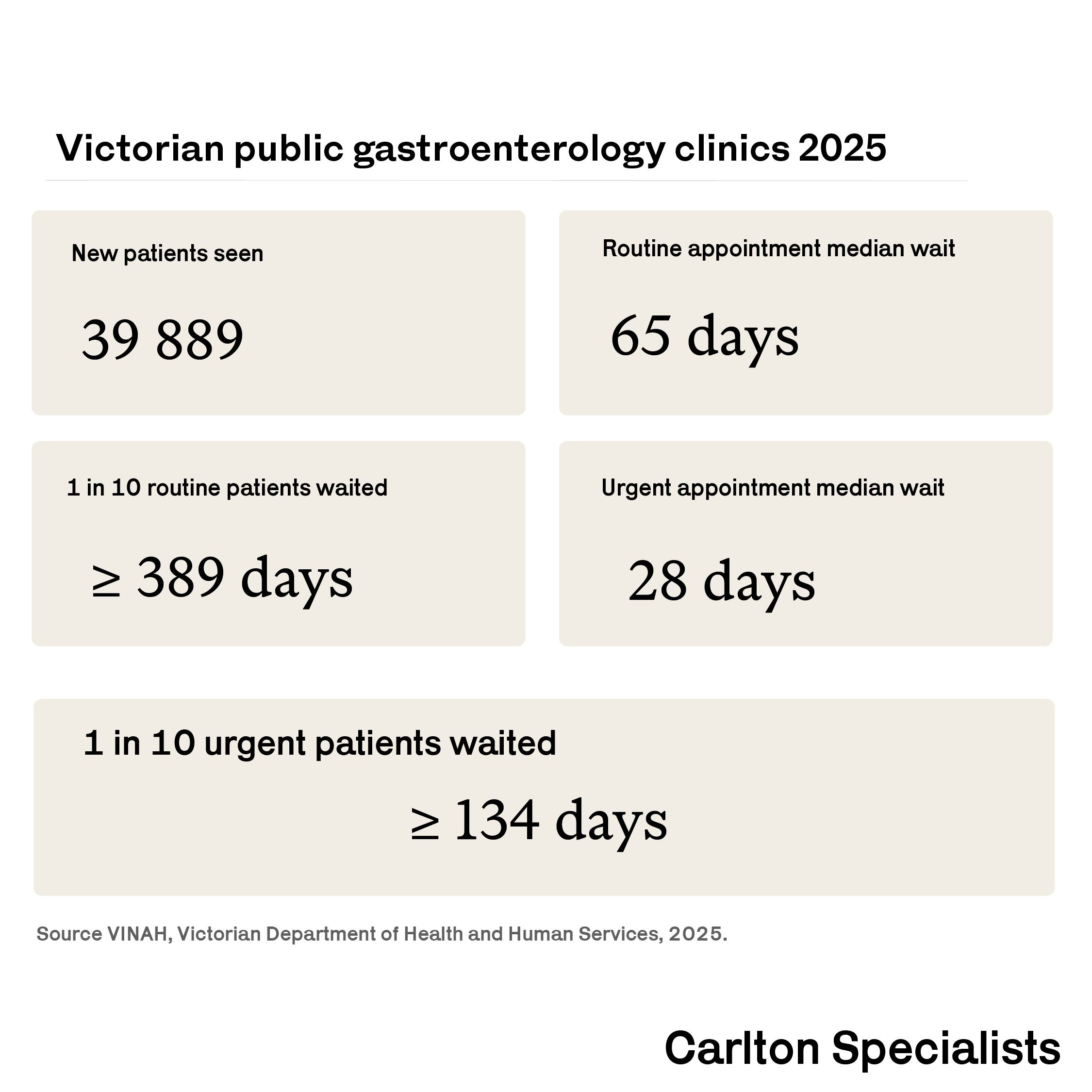
Data from the Victorian Integrated Non-Admitted Health Dataset (VINAH), Victorian Department of Health and Human Services, show that in 2025 the median wait for a routine first gastroenterology appointment in the Victorian public system was 65 days. One in ten patients waited 389 days or more. Even patients referred as urgent waited a median of 28 days for their first appointment, with one in ten waiting more than four months.
Some presentations don’t meet the criteria for public hospital acceptance, not because they are unimportant, but because they fall below the acuity threshold the public system is resourced to manage.
Private gastroenterology exists in part to serve patients in these situations, whether that means faster access to assessment, or care for presentations that wouldn’t be accepted by a public service. For many patients, private care also means a more predictable timeline. If you have private health insurance, your insurer may cover some or all of the costs of inpatient procedures (e.g. gastroscopy, colonoscopy). For outpatient consultations, a Medicare rebate applies with a valid GP referral regardless of whether you hold private insurance.
Wait time data is sourced from the Victorian Agency for Health Information (VAHI) Specialist Clinics dataset, filtered for gastroenterology outpatient appointments across Victorian public health services in 2025. Data is reported quarterly; overall 2025 figures represent the median of four quarterly medians, which is an approximation — precise annual medians would require individual patient-level data. Urgent and routine appointment categories are as defined by VAHI. Data for some smaller services was suppressed for privacy reasons and excluded from calculations.
What Happens at Your First Gastroenterology Appointment?
Your first appointment with a specialist can be daunting. In practice, a first gastroenterology consultation is a conversation more than anything else. The purpose of a consultation is to demystify symptoms and give clarity regarding the cause and next steps.
Before your appointment
You will need a referral from your GP, which also ensures you receive Medicare rebates for the consultation. It is worth bringing any recent test results, including blood tests, imaging, or previous endoscopy reports (and histology reports if available), as well as a list of your current medications.
The consultation itself
Your gastroenterologist will take a detailed history of your symptoms, your general medical background, and any relevant family history. A physical examination is usually performed. The appointment is an opportunity to ask questions, so it is worth writing them down beforehand.
Further investigations
Depending on your symptoms, your gastroenterologist may recommend blood tests, stool tests, imaging, or an endoscopic procedure such as a gastroscopy or colonoscopy. Not everyone needs a procedure at the outset. Some people are managed with medication or dietary changes after an initial consultation, with investigations arranged only if needed.
If a procedure is recommended
A gastroscopy involves a thin, flexible camera being passed through the mouth to examine the oesophagus, stomach, and upper small bowel. A colonoscopy examines the large bowel. Both are performed under sedation in hospital, so you won’t be awake for the procedure itself. You will receive specific preparation instructions beforehand, and you will need someone to drive you home afterwards. Results are typically discussed with you at a follow-up appointment.
Ongoing care
For straightforward conditions, a single consultation and investigation may be all that is required. For more complex or chronic conditions such as IBD or liver disease, care is ongoing and involves regular review with your gastroenterologist, often in coordination with your GP. Your specialist will communicate findings and recommendations back to your GP so that your care remains joined up.
This article is intended for general educational purposes and does not constitute medical advice. Symptoms vary between individuals, and this information should not replace a consultation with a qualified healthcare professional.
